
It is widely acknowledged by many in the health advisory field that excess build up of body fat accompanied by decreased insulin sensitivity referred to as insulin resistance (IR) have become quite common occurrences among the general public –- largely due to improper dietary preferences that favor intakes of too much sugar and excess calories [1]. This has, in turn, led to development of a number of metabolic risk factors commonly referred to as the metabolic syndrome (MS). The major related components of MS may include dyslipidemias (high triglyceride/low HDL-cholesterol circulating levels), elevated blood pressure, generalized inflammation and disturbed liver (excess fat infiltration) and kidney (lowered GFR) occurrences [1]. In another vein, previous practical and experimental findings imply that higher dietary calcium intakes may be associated with lower body weight [2,3] and improved optimal metabolic balances when it comes to MS [3].
In support of the latter possibility, it has been reported that diagnosed disorders like type 2 diabetes mellitus (T2DM), dyslipidemias, and hypertension have reportedly improved with augmented intake of dairy products [2]. Similar type investigations have shown both positive and negative results. These differences in interpretations may be caused by many factors including the amount and duration of intake, in addition to the age, gender, and initial starting point of scale weight. Recently, we reexamined this situation and corroborated that as the circulating levels of calcium rose, the bodily accumulation of fat decreased proportionately (Fig.1). Thus, our data corroborated some of the important previous findings.
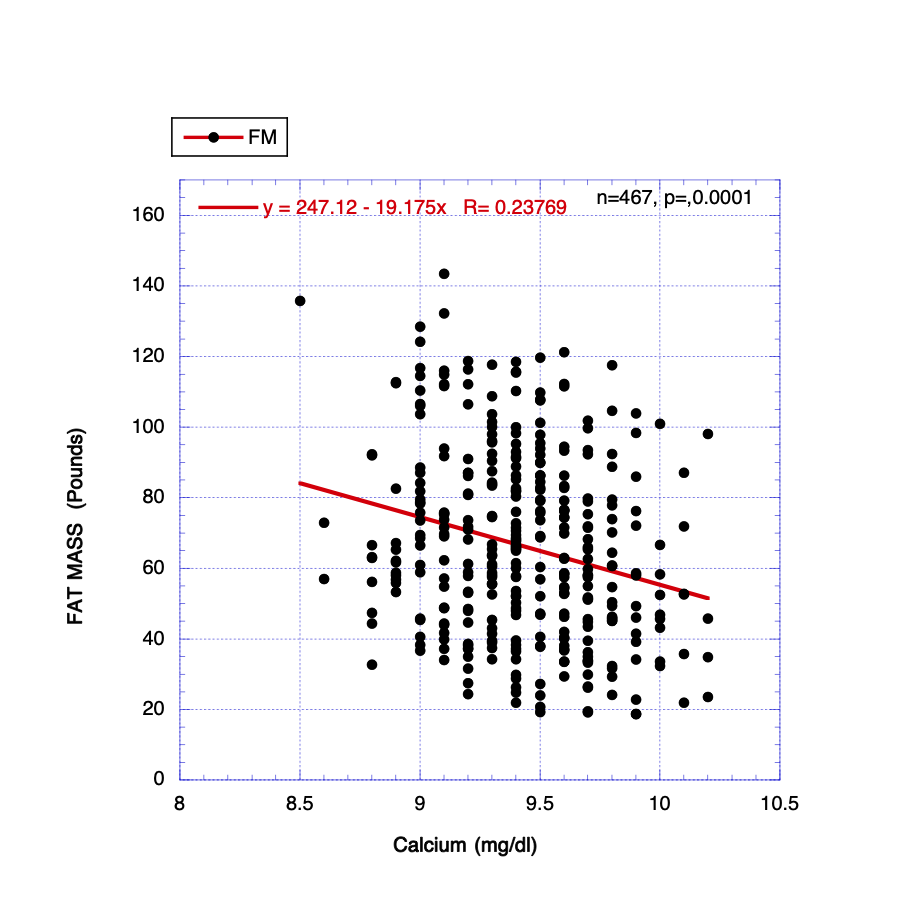
Fig.1 Calcium concentration vs. Fat Mass accumulation
However, a major medical trade-off was uncovered when examining rising levels of circulating calcium. As displayed above in a beneficial manner, higher calcium correlated significantly with lessened FM accumulation and serum overall evidence of inflammation, hsCRP concentrations. Unfortunately, on the negative side, rising calcium levels coincided with elevated values for LDL and non-HDL cholesterol, evidence suggesting enhanced hepatic fat infiltration, and markers intimating decreased renal function. Distinct from some previous reports, IR represented by FBG and changes in serum triglyceride concentrations were not influenced significantly by varying calcium status. So, circulating calcium levels correlate negatively with body fat mass accumulations but do not influence insulin aberrations to any significant extent. In addition, they remain relatively steady over the aging span and consequently appear not to participate extensively in that process.
Prior to utilizing means to supplement calcium intake to decrease body fat accumulation, the detrimental trade off manifestations must be taken under consideration.
Bibliography
- Preuss HG: The Bitter Sweet. Marcell Publishing, Columbia, SC, pp 1-116, 2017.
- Teegarden D: Calcium intake and reduction in weight or fat mass. J Nutr. 133: 249s-251s, 2003.
- Zemel MB, Richards J, Mathis S, Milstead A, Gebhardt A, Silva E: Dairy augmentation of total and central fat loss in obese subjects. Int J Obes London) 29:391-397, 2005.





{kind=link}
{kind=link}